Metabolic Health: Science Hub
Metabolic Health: Why 5 Signals Matter More Than the Number on Your Scale
Most metabolic health problems are not weight problems. They are signalling problems.
Written by Dr. Steven Gabriel, MD · Board-Certified Emergency Physician · Founder, BeyondGLP · June 2026
Metabolic health describes how well your body produces, uses, and stores energy—across appetite, blood sugar, digestion, sleep and recovery, and the hormones that regulate all of it. It is not the same as your weight: you can carry extra weight and still have healthy metabolic markers, or be at a “normal” weight with significant hidden metabolic dysfunction. Understanding what metabolic health means is the first step BeyondGLP helps you take, through the Metabolic Signaling System and a free metabolic assessment.
In this doctor-reviewed guide, Dr. Gabriel explains what metabolic health means, the five signal domains that drive it, and how to know where you stand.
Key Takeaways
- Metabolic health describes how well your body produces, uses, and stores energy across five signal domains: appetite, energy, digestion, sleep and recovery, and stress hormones.
- Weight and BMI are outputs of these signals — not measurements of metabolic function itself.
- Only 12.2% of US adults meet all criteria for optimal metabolic health, including many people who appear outwardly healthy and have normal standard lab results.
- Metabolic dysfunction — the slow deterioration of these signals — is the common upstream factor in type 2 diabetes, cardiovascular disease, and accelerated biological ageing.
- The BeyondGLP Metabolic Assessment identifies which of your five signal domains may need attention — a starting point the scale cannot provide.
From Dr. Gabriel
“The question I ask when a patient walks in isn’t ‘what does the scale say?’ — it’s ‘how are your metabolic signals working?’ Two people can sit in front of me at the same weight, with similar lab panels, and have completely different metabolic realities underneath. One has stable blood sugar, good insulin sensitivity, and appetite hormones that function reliably. The other has insulin levels that have been rising for years, visceral fat accumulating around the organs, and hunger signals that have started working against them — none of which shows up as a red flag on a standard physical. Metabolic health is the name for what those differences actually are. It’s the thing the scale doesn’t measure, the annual bloodwork often misses, and — critically — the thing that determines where your health is heading long before a diagnosis appears.”
What metabolic health means — beyond BMI
Your weight is one output of deeper metabolic signals, not the whole story.
The word “metabolic” refers to metabolism: the complete set of processes your body uses to convert food into energy, regulate blood sugar, build and repair tissue, and keep every organ functioning. When these processes work in balance, the result is metabolic health—stable energy, reliable hunger signals, consistent blood sugar, and body composition that reflects your actual health.
BMI measures the ratio of weight to height. It says nothing about where fat is stored, how well insulin is functioning, whether blood sugar is stable after meals, or how efficiently muscle tissue is being maintained. According to the National Institute of Diabetes and Digestive and Kidney Diseases, insulin sensitivity is the central mechanism of metabolic health: when the body uses insulin efficiently, glucose is cleared from the bloodstream reliably, appetite signals work as designed, and energy is stored and released appropriately. A cross-sectional analysis of 8,721 US adults found that only 12.2% meet all criteria for optimal metabolic health—with poor metabolic function present across every weight category, including normal-weight individuals (Araújo et al., PMID 30484738).
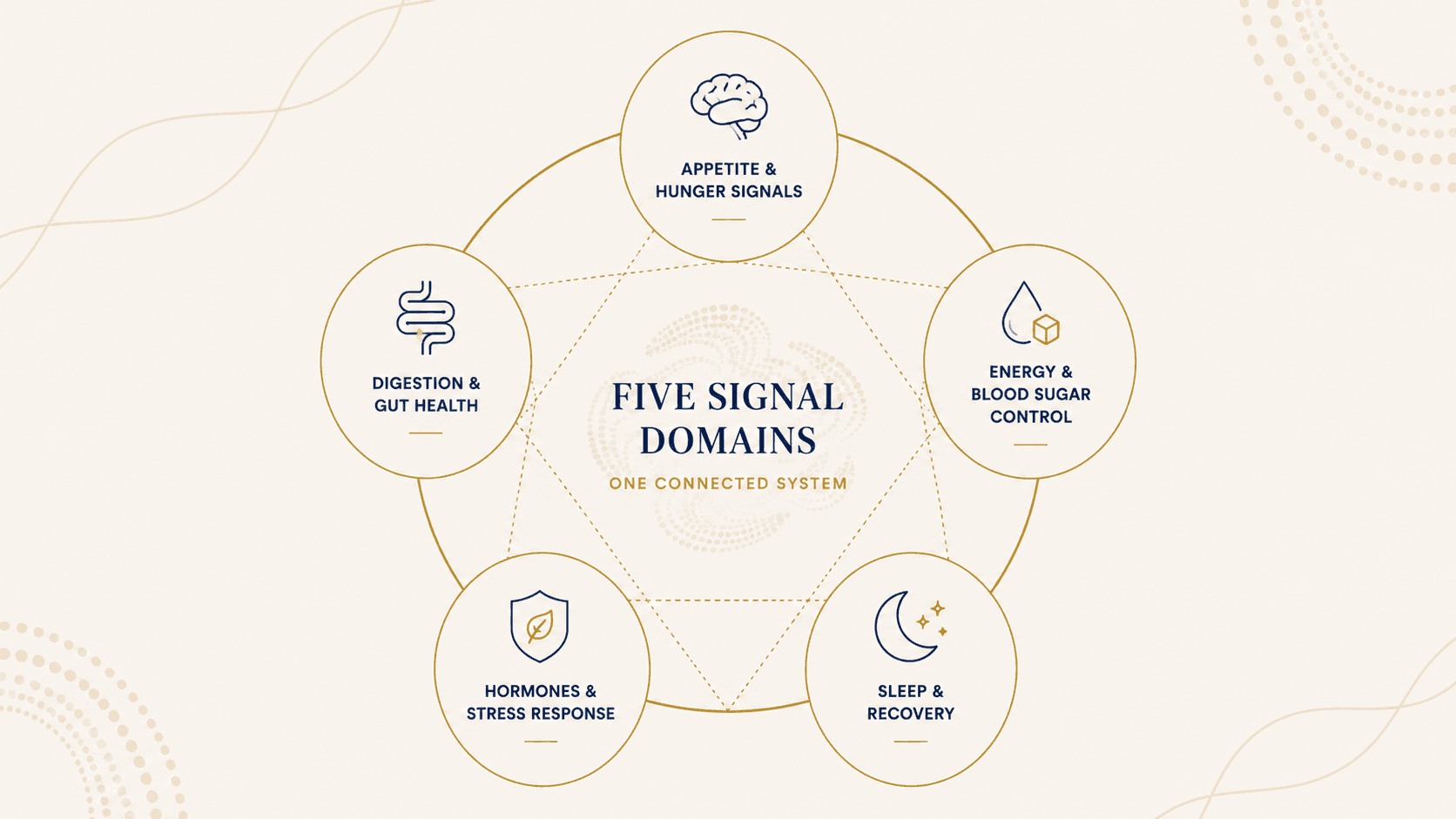
The five signal domains: what metabolic health actually measures
BeyondGLP organises metabolic health around five interconnected signal domains—the Metabolic Signaling System. Each domain influences the others.
Energy & Blood Sugar Control
After every meal, blood glucose rises. A healthy metabolic system clears it efficiently through insulin signalling, returning blood sugar to baseline within two hours. Insulin resistance—the gradual loss of this capacity—is the single most consequential metabolic dysfunction for long-term disease risk. It develops silently over years, typically while all standard lab values remain in the normal range.
Appetite & Hunger Signals
Hunger and satiety are governed by hormones—primarily GLP-1, leptin, ghrelin, and insulin. When these signals function correctly, hunger arises at appropriate times and meals produce reliable fullness. When disrupted by ultra-processed foods, insulin resistance, or hormonal changes, appetite becomes unreliable: hunger amplifies, satiety blunts, and cravings stop matching actual energy needs.
Digestion & Gut Health
The gut produces GLP-1—the same hormone GLP-1 medications mimic—in response to food. This signal travels to the brain to create satiety, to the pancreas to stimulate insulin, and to the stomach to slow digestion. When gut health is disrupted by ultra-processed food, dysbiosis, or low-grade inflammation, appetite regulation becomes unreliable from the gut upward.
Sleep & Recovery
Sleep deprivation acutely suppresses GLP-1 secretion, elevates ghrelin, and increases insulin resistance—compounding metabolic dysfunction from the top down. Recovery is not peripheral to metabolic health; it is a direct input to how well every other signal domain functions the following day.
Hormones & Stress Response
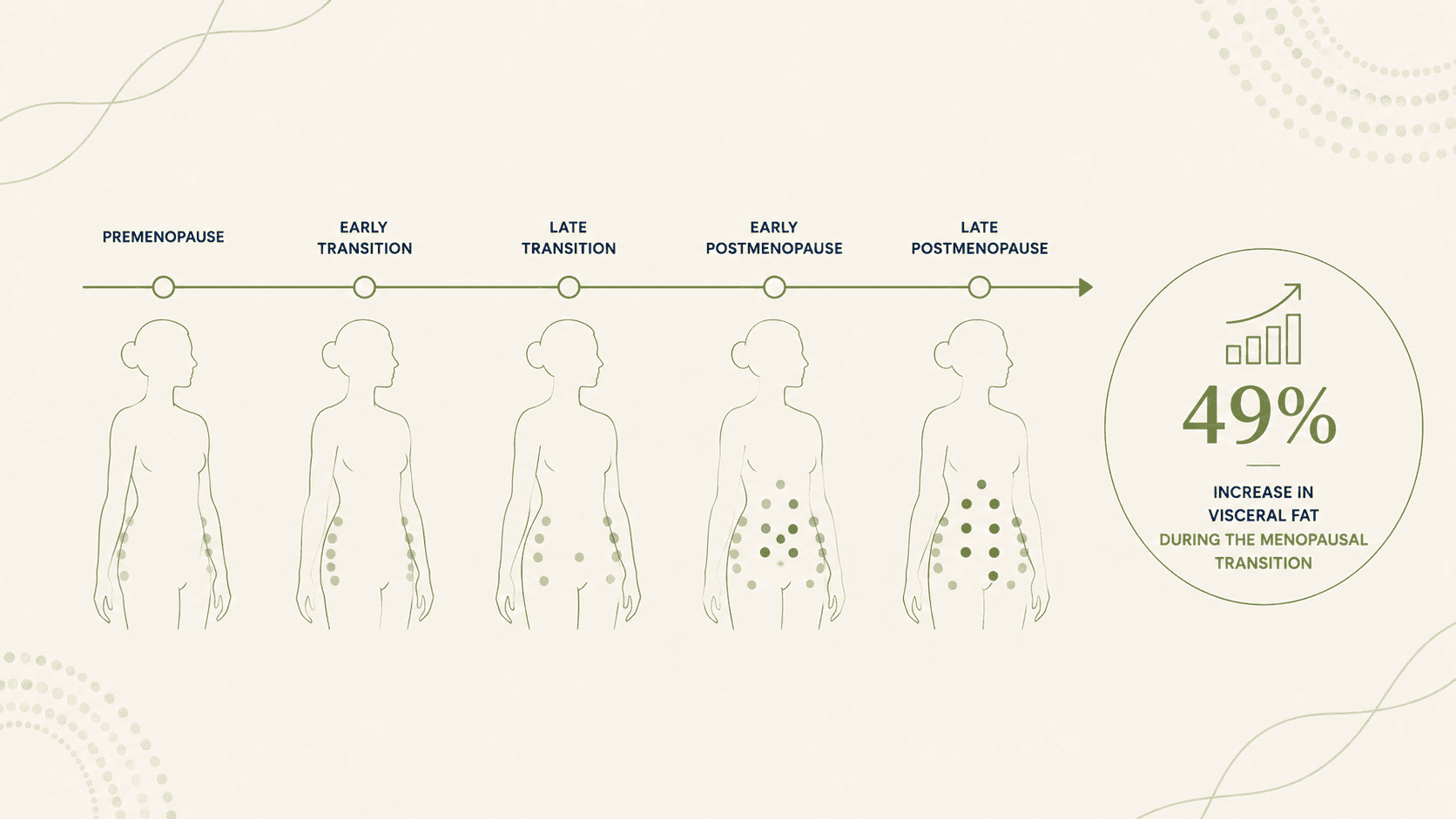
Reproductive hormones, thyroid function, and the stress axis (cortisol) intersect with every other metabolic signal. The menopausal transition produces a 49% increase in visceral fat independent of total weight change—and separately reduces postprandial GLP-1 secretion by 28%, partially explaining the increased appetite many women notice. These are biological changes, not failures of discipline.
Signs your metabolic health may need attention
Poor metabolic health rarely arrives as a diagnosis. It arrives as patterns—persistent, easy-to-explain-away symptoms that accumulate over months and years before any clinical threshold is crossed.
Energy and afternoon crashes
Blood sugar instability—glucose rising quickly after meals and dropping sharply 90–120 minutes later—is one of the most common but least recognised signs of impaired metabolic function. The afternoon energy drop that feels like it needs coffee or sugar to fix is often this pattern repeating daily.
Cravings that don't match hunger
When insulin sensitivity is reduced and blood sugar is volatile, the brain receives unreliable hunger signals. Cravings for carbohydrates and sugar—especially in the afternoon and evening—are frequently a symptom of dysregulated blood sugar, not insufficient willpower.
Weight that accumulates differently
When visceral fat—fat stored around the abdominal organs—begins to accumulate, body composition shifts in ways the scale often doesn't reflect clearly. Clothes fit differently. The waist measurement changes even when weight doesn't. This redistribution is one of the most reliable early signs of changing metabolic function.
Check Your Metabolic Profile →
Free · Physician-reviewed · Results in under 5 minutes
What is metabolic dysfunction and metabolic syndrome?
Metabolic dysfunction describes a state where one or more of the five signal domains are working below optimal capacity—often without yet meeting the threshold for a clinical diagnosis.
Metabolic syndrome is the clinical term for the advanced stage: the presence of three or more of five specific markers, as defined by the American Heart Association and NHLBI. These five commonly used clinical indicators are: abdominal obesity, elevated fasting triglycerides, reduced HDL cholesterol, elevated blood pressure, and elevated fasting glucose.
Meeting three of these five significantly elevates cardiovascular and metabolic disease risk. Metabolic dysfunction—the earlier and more widespread state—describes the years when signals are declining and markers are trending wrong, before standard medical care has found a reason to intervene. That gap between dysfunction and diagnosis is where early intervention is most effective.
Metabolic rate, metabolic age, and BMR
Basal metabolic rate (BMR) is the amount of energy the body uses at rest to sustain basic functions. The Mifflin–St Jeor equation is the most widely used clinical estimate. What BMR does not measure is metabolic health: a person can have a calculated BMR that looks normal and still have significant insulin resistance, poor blood sugar regulation, and accumulating visceral fat.
“Metabolic age” estimates how your BMR compares to population averages for your age—an estimate, not a diagnosis, and one that says nothing about the five signal domains that actually determine health trajectories. See Metabolic Rate, BMR and Metabolic Age Explained for a fuller picture.
How metabolic health changes with age, menopause, and GLP-1
Metabolic health is not static. It changes across the lifespan, and several biological transitions accelerate the pace of that change.
Age and muscle loss.According to the National Institute on Aging, adults begin losing muscle mass at approximately 3–5% per decade after age 30, with the rate accelerating after 60. Because skeletal muscle is the primary site of glucose uptake and the primary driver of resting metabolic rate, this progressive loss directly reduces insulin sensitivity and shifts the body’s response to food and weight management—independent of caloric intake.
Menopause and fat redistribution. A longitudinal cohort study published in the Journal of Clinical Endocrinology & Metabolism (2012) found that women experience a 49% increase in visceral fat during the menopausal transition, independent of total body weight change (Lovejoy et al., PMID 22240495). Research in Endocrine (2020) separately found that postmenopausal women have 28% lower postprandial GLP-1 secretion than premenopausal women of similar BMI (El Bekay et al., PMID 31637636). These are biological changes, not failures of discipline.
GLP-1 medications and metabolic context.GLP-1 receptor agonists—including semaglutide and tirzepatide—work by mimicking the gut’s natural GLP-1 signal. They are most effective when metabolic foundations are in place: protein intake to protect lean mass and habits that support insulin sensitivity. BeyondGLP’s GLP-1 content is informational only—any decisions about medication should be made with a licensed prescriber.
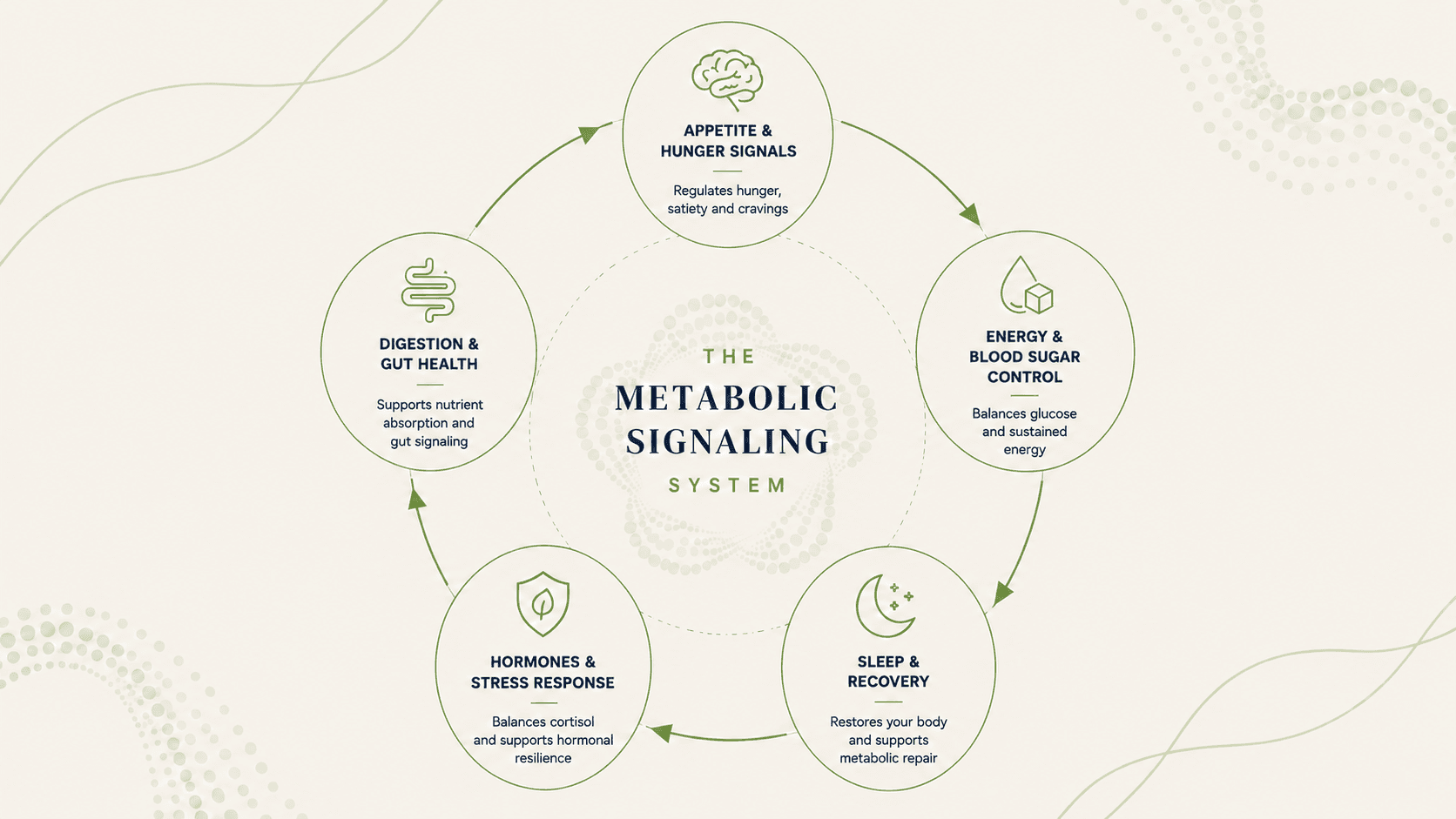
The BeyondGLP approach: the Metabolic Signaling System
BeyondGLP was built on one clinical observation: most metabolic health problems are not weight problems. They are signalling problems.
The Metabolic Signaling System frames the five biological signal domains as an interconnected system. When one signal is disrupted, the others compensate—which is why metabolic dysfunction rarely presents as a single symptom. It presents as a cluster: fatigue, cravings, changing body composition, disrupted sleep, with no obvious single cause. The framework organises BeyondGLP’s assessment and protocol around the same logic: understand the signals, identify which are disrupted, address them in order.
How to assess your own metabolic health
A standard annual physical assesses fasting glucose and basic lipids. It rarely captures fasting insulin, waist circumference, the triglyceride-to-HDL ratio, or any measure of gut-brain axis function—the markers most sensitive to early dysfunction.
The BeyondGLP Metabolic Assessment evaluates all five signal domains through a structured profile, producing a personalised MetaScore that identifies which signals need attention and in what order. It does not replace clinical evaluation or laboratory testing. It is a starting point: the picture your annual physical doesn’t give you.
3 Articles in This Hub
1→
Foundation
What Is Metabolic Health? A Plain-English Definition
What metabolic health actually means, the five clinical markers clinicians look at, and why weight alone doesn't capture the full story.
7 min read
2→
Dysfunction
Metabolic Dysfunction and Metabolic Syndrome: What They Mean and Why the Difference Matters
Your bloodwork can look normal for years while metabolic dysfunction builds quietly. The difference between dysfunction and syndrome, and where the most leverage exists.
6 min read
3→
Metabolic Rate
Metabolic Rate, BMR, and Metabolic Age: What They Measure — and What They Miss
BMR tells you how much energy your body uses at rest. A plain-English guide to what the equation captures, what metabolic age actually means, and what neither tells you.
6 min read
Common Questions
Can you be metabolically healthy at any weight?
Yes — and this distinction matters more than most people realise. Research consistently shows that metabolic dysfunction is not confined to people who are overweight, and metabolic health is not guaranteed by a normal BMI. A 2019 analysis of 8,721 US adults found that only 12.2% were fully metabolically healthy — with poor metabolic function present across every weight category, including normal-weight individuals (Araújo et al., PMID 30484738).
How is metabolic health different from weight loss?
Weight loss is a potential outcome of improved metabolic health — but it is not the same thing. Metabolic health addresses the signals that govern how the body processes food, regulates blood sugar, maintains lean mass, and controls hunger. When those signals improve, weight often normalises — but the reverse is not reliably true. Pursuing weight loss through caloric restriction without addressing the underlying signals tends to produce temporary results.
What is the difference between metabolic health and metabolic syndrome?
Metabolic health describes the overall functional state of the body's energy systems — a spectrum from optimal to severely disrupted. Metabolic syndrome is a specific clinical diagnosis defined by the American Heart Association as the presence of three or more of five markers (waist circumference, blood pressure, fasting glucose, triglycerides, HDL cholesterol) outside their optimal ranges. You can have significant metabolic dysfunction — declining signals, trending markers — without yet meeting the threshold for metabolic syndrome. That gap is exactly where early intervention is most effective.
How do I check my metabolic health?
The full picture includes fasting blood glucose, fasting insulin, blood pressure, waist circumference, fasting triglycerides, and HDL cholesterol. Standard annual bloodwork captures some of this — but fasting insulin and waist circumference are rarely included, and they carry significant early-detection weight. The BeyondGLP Metabolic Assessment evaluates all five signal domains — energy and blood sugar control, appetite and hunger signals, digestion and gut health, Sleep & Recovery, and hormones and stress response — and produces a personalised baseline.
Scientific References
- 1.Araújo J, Cai J, Stevens J. Prevalence of optimal metabolic health in American adults: National Health and Nutrition Examination Survey 2009–2016. Metabolic Syndrome and Related Disorders, 2019. PMID 30484738. pubmed.ncbi.nlm.nih.gov/30484738/
- 2.Petersen MC, Shulman GI. Mechanisms of insulin resistance: cellular and molecular pathways. Diabetologia, 2021. PMID 34091725. pubmed.ncbi.nlm.nih.gov/34091725/
- 3.Drucker DJ. Mechanisms of action and therapeutic application of glucagon-like peptide-1. Cell Metabolism, 2018. PMID 29617641. pubmed.ncbi.nlm.nih.gov/29617641/
- 4.Grundy SM, Cleeman JI, Daniels SR, et al. Diagnosis and management of the metabolic syndrome: an AHA/NHLBI scientific statement. Circulation, 2005. PMID 16157765. pubmed.ncbi.nlm.nih.gov/16157765/
- 5.Lovejoy JC, Champagne CM, de Jonge L, Xie H, Smith SR. Increased visceral fat and decreased energy expenditure during the menopausal transition. Journal of Clinical Endocrinology & Metabolism, 2012. PMID 22240495. pubmed.ncbi.nlm.nih.gov/22240495/
- 6.El Bekay R, Coín-Aragüez L, Fernández-García D, et al. Oestrogen decline and postprandial GLP-1 secretion in menopausal women. Endocrine, 2020. PMID 31637636. pubmed.ncbi.nlm.nih.gov/31637636/
- 7.National Institute on Aging, NIH. Metabolism and Weight Loss: How Metabolism Changes as You Age. www.nia.nih.gov/health/body-weight-and-obesity/metabolism-and-weight-loss-how-metabolism-changes-age
Connected Science
Ultra-Processed Foods
How ultra-processed foods disrupt the metabolic signals that govern hunger, fullness, and fat storage.
GLP-1 Science
How GLP-1 supports appetite control, satiety, and metabolic health, and what the research actually shows.
Food Noise and Appetite
What food noise is, why it happens, and how appetite signals drive it.
The BeyondGLP System
The Metabolic Signaling System framework: how BeyondGLP structures assessment and support across the five signal domains.
Take the Metabolic Assessment →
Free · Physician-reviewed · See which of your five signal domains may need attention
Educational content only. Information explains physiology and is not intended as medical advice. Always consult a qualified healthcare provider regarding medical decisions.