Metabolic Health · Article 3 of 3
Metabolic Rate, BMR, and Metabolic Age: What They Measure — and What They Miss
BMR tells you how much energy your body uses at rest. It doesn't tell you how well your metabolism is actually working.
Written by Dr. Steven Gabriel, MD · Board-Certified Emergency Physician · June 2026
Key Takeaways
- Basal metabolic rate (BMR) is an estimate of how much energy your body uses at rest. It is useful as a baseline — but it is not a measure of metabolic health.
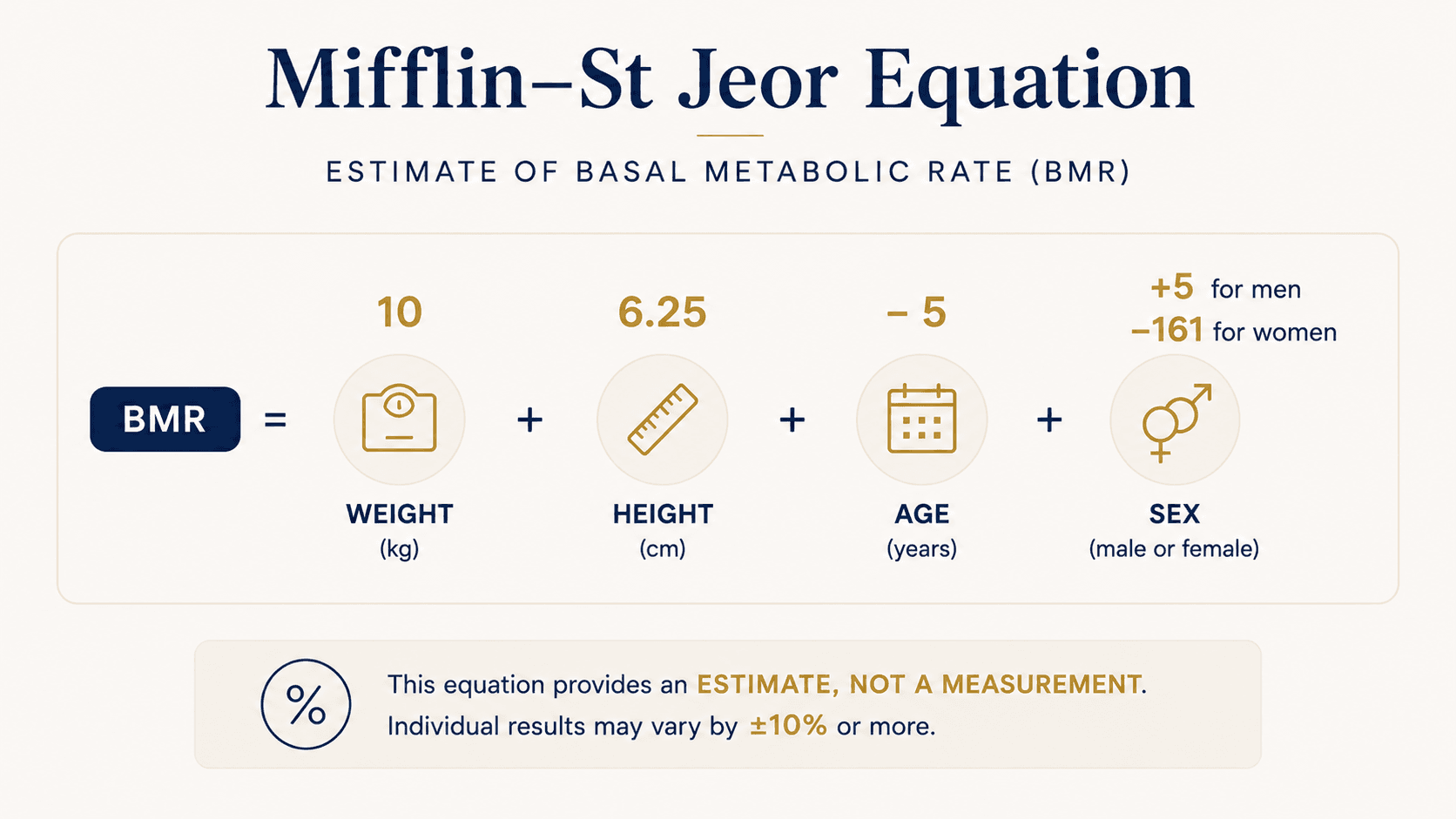
- The Mifflin–St Jeor equation, the most widely used BMR formula, was validated on 498 adults in 1990 and carries an individual error margin of approximately ±10%.
- A person can have a normal calculated BMR and still have significant insulin resistance, poor blood sugar regulation, and accumulating visceral fat.
- "Metabolic age" is a population-comparison estimate, not a clinical measurement. It describes where your BMR sits relative to averages — not how well your five signal domains are functioning.
- The BeyondGLP Metabolic Assessment evaluates the five signal domains standard metabolic rate calculations cannot reach: appetite, energy, digestion, sleep and recovery, and stress hormones.
From Dr. Gabriel
“I have patients who come in asking about their metabolic age — they’ve entered their stats into an app and been told they have the metabolism of a 55-year-old when they’re 42. Sometimes the result concerns them. Sometimes it reassures them. But the number doesn’t mean what they think it means. BMR is a useful rough estimate of energy expenditure. It tells you approximately how many calories your body burns keeping you alive. What it doesn’t tell you is whether your insulin is working efficiently, whether your blood sugar is crashing at 3pm, whether your gut is producing the GLP-1 signals your appetite system needs, or whether your cortisol is running high enough to be driving visceral fat deposition independently of what you eat. Metabolic rate and metabolic health are related but they’re not the same thing, and that’s important because it leads people to optimize for the wrong number.”
You’ve probably seen a BMR calculator — a tool that takes your height, weight, age, and sex and produces a number representing how many calories your body burns at rest. You may have also encountered the concept of “metabolic age” — a comparison of your BMR against population averages. These are useful estimates. They are not measures of metabolic health. Understanding what metabolic rate measures, how it’s calculated, where it falls short, and how it relates to the broader picture of metabolic function will help you use these numbers correctly — and know what they don’t tell you.
What is metabolic rate?
Metabolic rate is the speed at which your body converts food and stored energy into the fuel needed to maintain basic biological functions.
At the most fundamental level, your body needs energy continuously — to keep the heart beating, lungs breathing, brain functioning, organs operating, and cells repairing. This continuous baseline energy expenditure is called basal metabolic rate, or BMR. It accounts for approximately 60 to 70% of total daily energy expenditure in sedentary adults.
Above BMR, additional energy is used for digestion (the thermic effect of food, roughly 10% of daily expenditure) and physical activity (variable, but typically 20–30% in moderately active adults). Total daily energy expenditure is the sum of all three components.
Basal metabolic rate (BMR)
Energy expenditure under strict resting conditions — lying still, in a thermally neutral environment, after an overnight fast, in a post-absorptive state. It is the minimum energy required to sustain basic physiological function.
Resting metabolic rate (RMR)
Measured under less strict conditions and approximately 10–20% higher than BMR. Most online calculators and fitness devices estimate RMR, not true BMR, and use the terms interchangeably.
Metabolic rate (everyday usage)
The perceived speed of a person's metabolism — how efficiently the body manages energy, weight, and body composition. A "fast metabolism" and a "slow metabolism" describe the experience of energy management, not a single measurable value.
How BMR is calculated — and what the equation actually measures
The most widely used method for estimating BMR is the Mifflin–St Jeor equation, developed and validated in a study of 498 healthy adults published in the American Journal of Clinical Nutrition in 1990 (Mifflin et al., PMID 2305711).
Three things are important to understand about what this equation does and does not measure:
First, it is a population-derived estimate with meaningful individual variability. The study validation showed a mean prediction error of approximately ±10% for most individuals — meaning a calculated BMR of 1,600 calories per day could reflect an actual BMR anywhere from approximately 1,440 to 1,760 calories in a real person.
Second, it uses only four variables — weight, height, age, and sex. It says nothing about body composition (muscle vs fat), insulin sensitivity, hormonal status, gut health, or any of the other biological factors that determine how efficiently the body actually uses energy.
Third, it estimates resting energy expenditure only. It does not account for blood sugar regulation quality, the efficiency of insulin signalling, the reliability of appetite hormones, or how the body partitions energy between fat storage and active use.
What is metabolic age?
Metabolic age is a comparison of your calculated BMR against average BMR values for people of your actual age in the general population.
If your calculated BMR is higher than the average for your age group, your metabolic age is reported as younger than your chronological age. If your BMR is lower than average, your metabolic age is reported as older.
Because metabolic age is derived from BMR, it inherits all the limitations of that calculation — particularly the ±10% individual error margin, the absence of body composition data, and the inability to capture insulin sensitivity, hormonal status, or gut function. Two people with identical metabolic ages can have radically different actual metabolic health profiles: one with excellent insulin sensitivity, stable blood sugar, and well-functioning appetite signals; the other with significant insulin resistance, poor blood sugar regulation, and declining GLP-1 output.
Metabolic age is an estimate of where your energy expenditure sits relative to a population average. It is not a diagnosis. It is not a measure of how well your five signal domains are functioning. Treating it as one leads to a false sense of either security or concern.
Why BMR alone doesn’t capture metabolic health
Metabolic health — the overall functional state of the body’s energy systems — is determined by five interconnected signal domains: Appetite & Hunger Signals, Energy & Blood Sugar Control, Digestion & Gut Health, Sleep & Recovery, and Hormones & Stress Response.
BMR captures a portion of one of these — the energy expenditure component of Energy & Blood Sugar Control. It misses almost everything else.
A person can have a calculated BMR that looks entirely normal and still have:
Significant insulin resistance
The gradual loss of cellular insulin sensitivity that typically develops over 10–15 years before producing abnormal fasting glucose values. Research published in Physiological Reviews (2018) established that insulin resistance develops through ectopic lipid accumulation, chronic inflammation, and mitochondrial dysfunction — none of which affects BMR calculation (Petersen & Shulman, PMID 30067154).
Elevated fasting insulin
Which predicts cardiovascular disease onset approximately 10 years earlier than elevated fasting glucose in prospective cohort data, but is not captured by any metabolic rate calculation (Salazar et al., Atherosclerosis, 2020 — PMID 24132974).
Accumulating visceral fat
Which is metabolically active in ways subcutaneous fat is not, and which correlates poorly with BMI or total body weight. Waist circumference is the more predictive measure of visceral fat accumulation — and it does not appear in any BMR equation.
Disrupted appetite signalling
GLP-1 function, leptin sensitivity, and ghrelin patterns that determine hunger reliability have no relationship to resting energy expenditure.
Check Your Metabolic Profile →
Free · Physician-reviewed · Results in under 5 minutes
How metabolic rate changes with age — and what that means
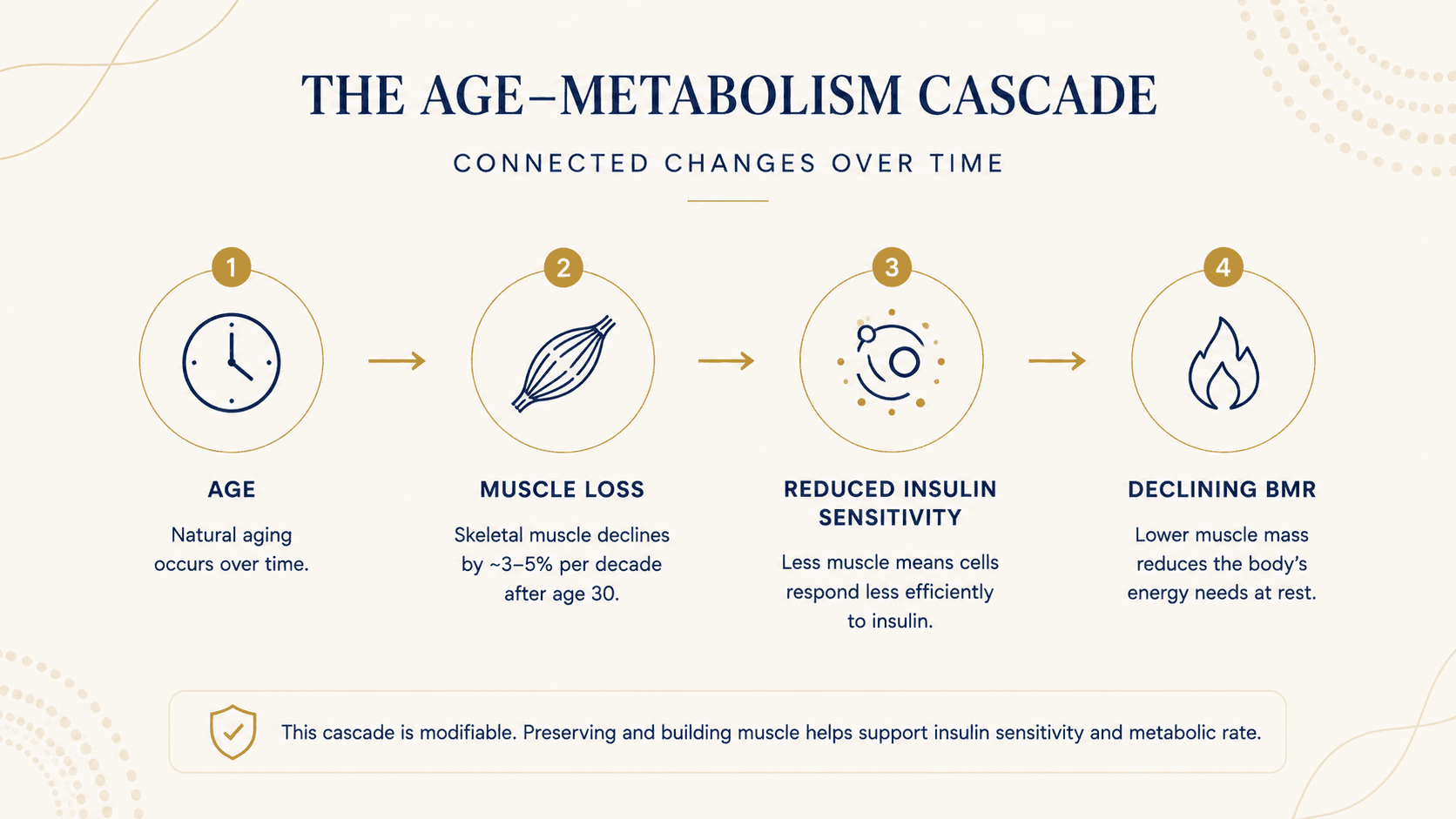
According to the National Institute on Aging, adults begin losing muscle mass at approximately 3–5% per decade after age 30, with the rate accelerating after 60. Because skeletal muscle is the primary site of insulin-mediated glucose uptake and the primary driver of resting metabolic rate, this progressive loss produces two compounding effects: a gradual decline in BMR (reflecting less metabolically active tissue) and a direct reduction in insulin sensitivity (reflecting less capacity for glucose uptake).
This is the biological mechanism behind the common experience of weight management becoming harder with age despite no major changes in diet or activity. It is not primarily a calorie story. It is a muscle and insulin sensitivity story.
A declining BMR with age is expected and normal. It does not indicate metabolic disease. What matters is whether the five signal domains are functioning well alongside that declining BMR — whether blood sugar remains stable, appetite signals remain reliable, gut health supports GLP-1 production, sleep restores metabolic function, and stress hormones remain appropriately regulated.
How to know where your metabolism actually stands
A BMR calculation gives you one number from one domain. It does not tell you whether your insulin is working efficiently, whether your gut is producing adequate GLP-1, whether your cortisol is silently driving visceral fat deposition, or whether your sleep is restoring the metabolic function it should.
The BeyondGLP Metabolic Assessment evaluates all five signal domains — Appetite & Hunger Signals, Energy & Blood Sugar Control, Digestion & Gut Health, Sleep & Recovery, and Hormones & Stress Response — through a structured self-reported profile, producing a personalised MetaScore that identifies which signals may need attention and in what order. It is not a diagnostic tool and does not replace clinical evaluation or laboratory testing.
Common Questions
Is a higher metabolic rate always better?
Not necessarily. A higher BMR means your body uses more energy at rest, which can support weight management — but BMR is only one component of metabolic health. A person can have a high calculated BMR and still have significant insulin resistance, poor blood sugar regulation, and disrupted appetite signals. The goal is not to maximise energy expenditure — it is for all five signal domains to function well together.
Does "slow metabolism" explain weight gain?
The phrase "slow metabolism" usually describes a combination of factors — declining insulin sensitivity, reduced muscle mass, disrupted appetite signalling, and changes in how the body partitions energy — rather than a single measurable value. BMR does decline gradually with age and muscle loss, but the experience of progressive weight management difficulty is more accurately a story about insulin resistance and signal domain disruption than about resting calorie burn alone.
Can you increase your metabolic rate?
BMR is primarily determined by lean muscle mass. Resistance exercise that builds or preserves skeletal muscle has the strongest evidence base for supporting resting metabolic rate. Adequate dietary protein is required to support this. Beyond muscle preservation, the more clinically significant question is often not how to increase BMR but how to improve insulin sensitivity, stabilise blood sugar, support GLP-1 function, and restore the signal domains that govern how efficiently the body uses the energy it has. BeyondGLP does not make specific outcome claims — your clinician can advise on what is appropriate for your situation.
What is the difference between BMR and RMR?
BMR is measured under strict fasting and resting conditions and represents the absolute minimum energy expenditure for basic biological function. RMR is measured under less strict conditions and is approximately 10–20% higher. Most online calculators estimate RMR, not true BMR, though the terms are commonly used interchangeably.
How accurate are online BMR calculators?
The Mifflin–St Jeor equation used by most calculators has a mean prediction error of approximately ±10% for most individuals. That means a calculated BMR of 1,600 calories could reflect an actual value anywhere from roughly 1,440 to 1,760 calories. Individual variation due to genetics, body composition, hormonal status, and mitochondrial efficiency is substantial and cannot be captured by a four-variable equation.
Scientific References
- 1.Mifflin MD, St Jeor ST, Hill LA, Scott BJ. A new predictive equation for resting energy expenditure in healthy individuals. American Journal of Clinical Nutrition, 1990. PMID 2305711. pubmed.ncbi.nlm.nih.gov/2305711/
- 2.Petersen MC, Shulman GI. Mechanisms of insulin resistance: cellular and molecular pathways. Diabetologia, 2021. PMID 30067154. pubmed.ncbi.nlm.nih.gov/30067154/
- 3.Salazar MR, Carbajal HA, Espeche WG, et al. Fasting insulin as a marker to predict the onset of cardiometabolic diseases: a 15-year prospective study. Atherosclerosis, 2020. PMID 24132974. pubmed.ncbi.nlm.nih.gov/24132974/
- 4.National Institute on Aging, National Institutes of Health. Metabolism and Weight Loss: How Metabolism Changes as You Age. www.nia.nih.gov/health/body-weight-and-obesity/metabolism-and-weight-loss-how-metabolism-changes-age
- 5.Harris JA, Benedict FG. A Biometric Study of Human Basal Metabolism. Proceedings of the National Academy of Sciences, 1918. (Historical reference — Harris–Benedict equation context.) pubmed.ncbi.nlm.nih.gov/16576330/
Take the Metabolic Assessment →
See which of your five signal domains may need attention
Educational content only. Information explains physiology and is not intended as medical advice. Always consult a qualified healthcare provider regarding medical decisions.