Metabolic Health · Article 2 of 3
Metabolic Dysfunction and Metabolic Syndrome: What They Mean and Why the Difference Matters
Your bloodwork can look normal for years while metabolic dysfunction builds quietly underneath.
Written by Dr. Steven Gabriel, MD · Board-Certified Emergency Physician · June 2026
Key Takeaways
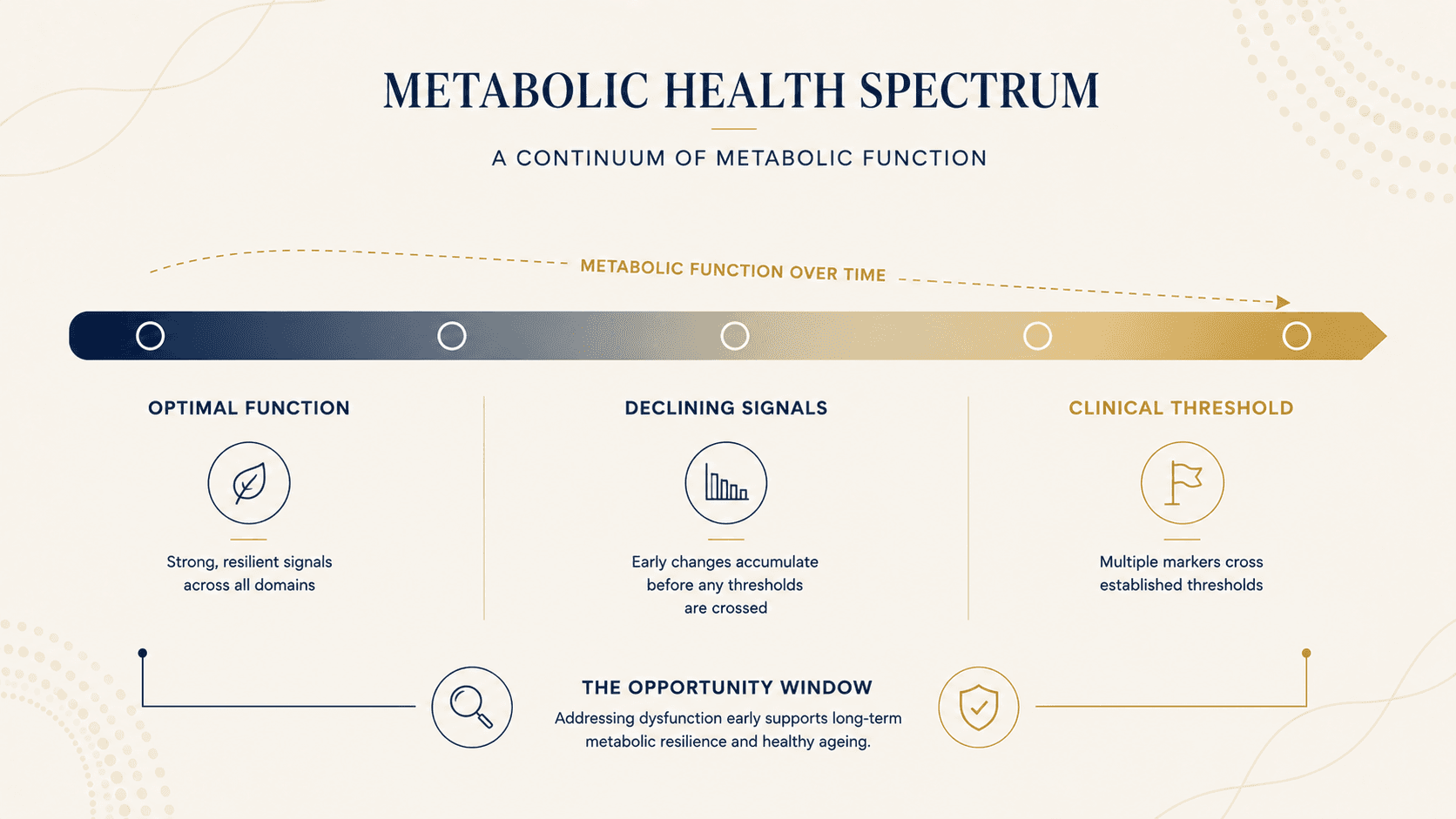
- Metabolic dysfunction describes declining signal domains before any clinical threshold is crossed — it is the years between optimal function and a formal diagnosis.
- Metabolic syndrome is a specific clinical diagnosis: three or more of five AHA/NHLBI criteria simultaneously present. It meaningfully elevates cardiovascular and type 2 diabetes risk.
- The most consequential dysfunction — insulin resistance — typically develops over 10 to 15 years with normal-appearing standard labs.
- Poor metabolic health is not confined to people who are overweight. It appears across all BMI categories, including normal-weight adults.
- The BeyondGLP Metabolic Assessment evaluates five signal domains — Appetite & Hunger Signals, Energy & Blood Sugar Control, Digestion & Gut Health, Sleep & Recovery, and Hormones & Stress Response — to identify dysfunction before it becomes a diagnosis.
From Dr. Gabriel
“In the emergency department, I see the end result of a decade of metabolic dysfunction — the heart attack, the stroke, the diabetes. What I didn’t see was the 10 years that led to those life-threatening diseases: the slow insulin rise, the expanding waist, the blood pressure trending upward. Medicine is good at catching crises. It is not good at catching the early-stage dysfunction that leads to them. Metabolic dysfunction is that early stage — the biological state where signals are declining, markers are trending wrong, and the body is compensating in ways that eventually stop working. By the time it shows up as a diagnosis, the window for low-effort intervention has usually closed. That gap — between normal labs and actual metabolic function — is exactly why I created BeyondGLP: to educate you before this happens.”
Metabolic dysfunction and metabolic syndrome are related but distinct concepts that are frequently confused — sometimes even in clinical settings. Understanding the difference matters because they sit at different points on the same spectrum, carry different clinical implications, and require different levels of urgency. Metabolic health describes the optimal end of that spectrum. This article covers what happens when it deteriorates, what clinical medicine defines as the threshold for metabolic syndrome, and why the years of dysfunction before that threshold are where the most leverage exists.
What is metabolic dysfunction?
Metabolic dysfunction describes a state where one or more of the five signal domains are working below optimal capacity — without yet meeting the threshold for a clinical diagnosis.
It is not a single condition. It is a direction of travel. Insulin sensitivity declining gradually. Blood sugar taking longer to clear after meals. Visceral fat accumulating while BMI stays stable. Appetite signals becoming less reliable. Sleep quality eroding. Stress hormones staying elevated. None of these individually triggers a clinical response. Together, they describe a body compensating harder than it should — and moving toward a threshold it has not yet crossed.
According to the National Institute of Diabetes and Digestive and Kidney Diseases, insulin resistance — the reduced ability of cells to respond to insulin — is central to metabolic dysfunction. When insulin sensitivity declines, the pancreas compensates by producing more insulin to achieve the same glucose clearance. Blood sugar may remain normal while fasting insulin rises, silently, for years.
A prospective cohort study of 8,143 adults followed over 15 years found that elevated fasting insulin predicted cardiovascular disease onset approximately 10 years earlier than elevated fasting glucose (Salazar et al., Atherosclerosis, 2020 — PMID 24132974). Standard annual bloodwork measures glucose. It rarely measures insulin. That 10-year gap is where metabolic dysfunction lives — and where early intervention changes outcomes.
What is metabolic syndrome?
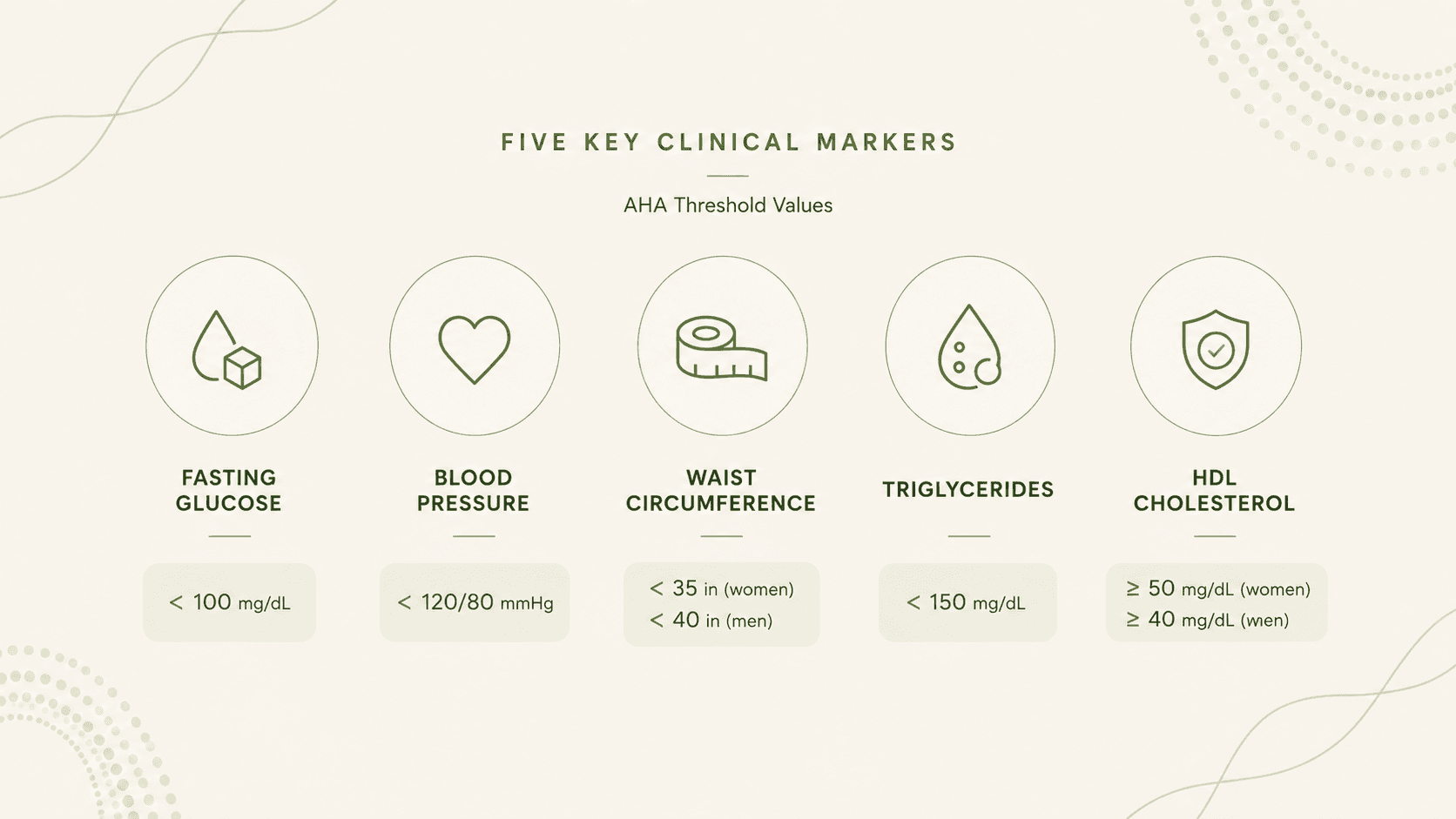
Metabolic syndrome is the clinical term for the advanced stage: the simultaneous presence of three or more of five specific criteria.
The American Heart Association defines metabolic syndrome as the presence of three or more of the following: abdominal obesity (waist circumference above 102cm in men or 88cm in women), elevated fasting triglycerides (≥150 mg/dL), reduced HDL cholesterol (below 40 mg/dL in men or 50 mg/dL in women), elevated blood pressure (≥130/85 mmHg), and elevated fasting glucose (≥100 mg/dL). This definition was established in the AHA/NHLBI 2005 scientific statement, which harmonised competing definitions from the WHO and the International Diabetes Federation into a single clinical standard (Grundy et al., Circulation, 2005 — PMID 16157765).
The clinical significance of meeting this threshold is not symbolic. A meta-analysis across 87 studies and 951,083 individuals found that metabolic syndrome is associated with a roughly 2-fold increase in cardiovascular outcomes and a 1.5-fold increase in all-cause mortality (Mottillo et al., Journal of the American College of Cardiology, 2010 — PMID 20863953). The combination of components produces risk greater than the sum of individual factors — confirming that the syndrome is a meaningful independent risk entity.
How insulin resistance drives both
Insulin resistance is the common upstream mechanism connecting metabolic dysfunction to metabolic syndrome.
According to research published in Physiological Reviews (2018), insulin resistance develops through ectopic lipid accumulation in the liver and skeletal muscle, chronic low-grade inflammation, and mitochondrial dysfunction. The process typically takes 10 to 15 years before producing abnormal standard lab values (Petersen & Shulman, PMID 30067154). During most of that period, fasting glucose remains within normal range, BMI may be unchanged, and a standard annual physical finds nothing to act on.
As insulin resistance progresses, the compensatory mechanisms begin to fail. The pancreas can no longer produce enough insulin to maintain normal glucose clearance. Blood pressure begins to rise. Triglycerides increase as the liver processes excess glucose into fat. HDL falls. Abdominal fat accumulates — particularly visceral fat, which is metabolically active in ways subcutaneous fat is not. The components of metabolic syndrome accumulate one by one, often over years, until three are present simultaneously and a clinical diagnosis is made.
The important clinical implication: insulin resistance precedes metabolic syndrome by a decade or more. Identifying it early — before any single marker crosses a clinical threshold — is where intervention is most effective.
The connection to the five signal domains
Metabolic dysfunction does not present as a single abnormal lab value. It presents as a pattern across multiple signal domains simultaneously.
Energy & Blood Sugar Control
Blood sugar instability — glucose rising sharply after meals and clearing more slowly than it should — produces the afternoon energy crashes and carbohydrate cravings that many people attribute to stress or poor sleep, not metabolic function.
Appetite & Hunger Signals
Insulin resistance impairs GLP-1 function and leptin sensitivity. Hunger signals become amplified; satiety signals become blunted. The experience of "food noise" — persistent intrusive thoughts about food between meals — is frequently a symptom of disrupted appetite signalling, not weak willpower.
Digestion & Gut Health
Gut microbiome composition influences GLP-1 secretion; disrupted gut health reduces the gut's capacity to produce the signals that regulate appetite and blood sugar.
Sleep & Recovery
Sleep deprivation acutely elevates cortisol, suppresses GLP-1, and increases insulin resistance — making poor sleep both a symptom and a cause of metabolic dysfunction. The relationship is bidirectional.
Hormones & Stress Response
Chronically elevated cortisol raises blood sugar independently of diet, drives visceral fat deposition, and blunts GLP-1 output. Metabolic dysfunction is rarely just a nutrition or exercise problem.
Who is at risk — and what the data shows
According to the Centers for Disease Control and Prevention, cardiometabolic risk factors are widespread in the US adult population and not confined to individuals who are visibly overweight or unwell.
A cross-sectional analysis of 8,721 US adults found that only 12.2% meet all five criteria for optimal metabolic health — and poor metabolic function appeared across all weight categories, including individuals of normal BMI (Araújo et al., Metabolic Syndrome and Related Disorders, 2019 — PMID 30484738). This means the vast majority of people with metabolic dysfunction do not look unwell, do not have flagged lab values, and are not receiving clinical intervention.
Risk factors that accelerate the progression of metabolic dysfunction include: ultra-processed food consumption, which impairs GLP-1 function and promotes insulin resistance; sedentary behaviour, which reduces insulin-mediated glucose uptake in skeletal muscle; chronic sleep disruption; chronic psychological stress; and the hormonal changes associated with ageing and the menopausal transition. None of these is individually catastrophic. In combination, over years, they compound.
What standard testing misses — and why
A standard annual physical typically includes fasting glucose and a basic lipid panel. These are useful. They are not sufficient.
Fasting insulin is rarely included in standard panels, despite being the most sensitive early marker of insulin resistance. Waist circumference — the most predictive anthropometric measure of visceral fat accumulation — is not routinely measured as a metabolic marker. The triglyceride-to-HDL ratio, which strongly correlates with insulin resistance, is available in standard bloodwork but rarely flagged or discussed unless both values are individually abnormal.
The result: a person can have elevated fasting insulin, a rising triglyceride-to-HDL ratio, increasing waist circumference, and two of the five metabolic syndrome criteria trending toward threshold — and receive confirmation that their bloodwork looks fine. This is not a failure of medicine. It is a limitation of what standard screening was designed to catch.
How to know where you stand
Understanding your metabolic function requires looking beyond the five clinical markers to the signal domains that standard testing cannot capture — appetite reliability, energy stability, digestion quality, sleep restoration, and stress hormone patterns.
The BeyondGLP Metabolic Assessment evaluates all five signal domains — Appetite & Hunger Signals, Energy & Blood Sugar Control, Digestion & Gut Health, Sleep & Recovery, and Hormones & Stress Response — through a structured self-reported profile, producing a personalised MetaScore that identifies which signals may need attention and in what order. It is not a diagnostic tool and does not replace clinical evaluation. It is a starting point: the picture your annual physical doesn’t give you.
Take the Metabolic Assessment →
Free · Physician-reviewed · Results in under 5 minutes
Common Questions
What is the difference between metabolic dysfunction and metabolic syndrome?
Metabolic dysfunction describes the broad spectrum of declining metabolic signal function — often present for years before any clinical marker crosses a threshold. Metabolic syndrome is a specific clinical diagnosis defined by the American Heart Association as the presence of three or more of five criteria: abdominal obesity, elevated triglycerides, reduced HDL, elevated blood pressure, and elevated fasting glucose. Significant dysfunction can exist — and should be addressed — before any formal diagnosis is made.
Can you have metabolic dysfunction without being overweight?
Yes. Research consistently shows that metabolic dysfunction, including insulin resistance, appears across all body weight categories. A 2019 analysis of 8,721 US adults found poor metabolic health present in normal-weight individuals. Waist circumference, not overall body weight, is the more predictive measure of visceral fat accumulation and metabolic risk (Araújo et al., PMID 30484738).
What causes metabolic dysfunction?
The primary drivers include insulin resistance (which develops through ectopic fat accumulation, chronic inflammation, and mitochondrial dysfunction over 10–15 years), ultra-processed food consumption, chronic sleep disruption, physical inactivity, chronic psychological stress, and hormonal changes associated with ageing and menopause. These factors interact and compound across all five signal domains.
Is metabolic dysfunction reversible?
BeyondGLP does not make disease-treatment claims. What the evidence supports is that metabolic signal function is modifiable through changes to nutrition, movement, sleep, and stress physiology — and that early intervention, before dysfunction reaches diagnostic thresholds, produces better outcomes than waiting for a diagnosis to act. Your clinician is the appropriate person to advise on your specific situation.
How is metabolic dysfunction detected early?
The most sensitive early markers are fasting insulin (not routinely included in standard panels), waist circumference, and the triglyceride-to-HDL ratio. In clinical settings, a comprehensive metabolic evaluation would include these alongside fasting glucose, blood pressure, and HDL. The BeyondGLP Metabolic Assessment adds the non-lab signal domains — appetite, digestion, sleep and recovery, and stress hormones — that laboratory testing cannot capture.
Scientific References
- 1.Araújo J, Cai J, Stevens J. Prevalence of optimal metabolic health in American adults: National Health and Nutrition Examination Survey 2009–2016. Metabolic Syndrome and Related Disorders, 2019. PMID 30484738. pubmed.ncbi.nlm.nih.gov/30484738/
- 2.Salazar MR, Carbajal HA, Espeche WG, et al. Fasting insulin as a marker to predict the onset of cardiometabolic diseases: a 15-year prospective study. Atherosclerosis, 2020. PMID 24132974. pubmed.ncbi.nlm.nih.gov/24132974/
- 3.Petersen MC, Shulman GI. Mechanisms of insulin resistance: cellular and molecular pathways. Diabetologia, 2021. PMID 30067154. pubmed.ncbi.nlm.nih.gov/30067154/
- 4.Grundy SM, Cleeman JI, Daniels SR, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute scientific statement. Circulation, 2005. PMID 16157765. pubmed.ncbi.nlm.nih.gov/16157765/
- 5.Mottillo S, Filion KB, Genest J, et al. The metabolic syndrome and cardiovascular risk: a systematic review and meta-analysis. Journal of the American College of Cardiology, 2010. PMID 20863953. pubmed.ncbi.nlm.nih.gov/20863953/
- 6.National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). Insulin Resistance and Prediabetes. www.niddk.nih.gov/health-information/diabetes/overview/what-is-diabetes/prediabetes-insulin-resistance
- 7.American Heart Association. About Metabolic Syndrome. www.heart.org/en/health-topics/metabolic-syndrome/about-metabolic-syndrome
- 8.Centers for Disease Control and Prevention. Adult Obesity Facts. www.cdc.gov/obesity/data/adult.html
Educational only. This page is for general education and is not medical advice, diagnosis, or treatment. Always consult a qualified healthcare provider regarding medical decisions. No outcomes are promised — individual results vary; nothing here guarantees weight loss or any specific health outcome. The BeyondGLP Metabolic Assessment is an educational metabolic profile, not a diagnostic device. Reviewed by Dr. Steven Gabriel MD on June 2026.