Insulin Resistance Explained: What It Is, How It Develops, and Why It Matters
Insulin resistance is the most consequential metabolic dysfunction most people have never been tested for.
Written by Dr. Steven Gabriel, MD · Board-Certified Emergency Physician · June 2026
Key Takeaways
- Insulin resistance is the gradual loss of cellular sensitivity to insulin — it typically develops over 10 to 15 years before producing abnormal standard lab values.
- During that decade, fasting glucose remains normal while fasting insulin rises silently — the most sensitive early marker that standard panels almost never measure.
- Insulin resistance is the common upstream mechanism connecting metabolic dysfunction to type 2 diabetes, cardiovascular disease, and metabolic syndrome.
- It is not confined to people who are overweight — it appears across all BMI categories and is driven by fat quality (visceral vs subcutaneous), not fat quantity.
- The BeyondGLP Metabolic Assessment evaluates the five signal domains — Appetite & Hunger Signals, Energy & Blood Sugar Control, Digestion & Gut Health, Sleep & Recovery, and Hormones & Stress Response — all of which are affected by insulin resistance.
From Dr. Gabriel
“In the emergency department I treat the diseases that were caused by years of insulin resistance — the heart attack, the stroke, the acute diabetes complication. But insulin resistance itself? I almost never see it presented to me as the problem. People don’t come into the ED saying ‘I think I’ve been developing insulin resistance for the past decade.’ They come in with the consequences. That’s the tragedy of how this condition works. It builds silently for years. The labs look normal. The patient feels reasonably well — maybe a bit more tired, maybe gaining some weight around the middle, maybe noticing that food doesn’t satisfy the way it used to. None of it rises to the level of a medical complaint. And then one day, it does. Catching insulin resistance before it produces consequences is exactly the kind of medicine we should all be doing more of — and it starts with understanding what it actually is.”
If there is a single concept that organises the science of metabolic health, it is insulin resistance. It underlies metabolic dysfunction, connects the five signal domains, and sits at the root of the most prevalent chronic conditions of modern life. Despite this, most people have never had their insulin measured — and many have never heard it explained in terms they can act on. This article covers what insulin resistance is, how it develops, what drives it, and why it is the metabolic variable worth understanding first.
What insulin does — and why resistance to it matters
Insulin is a hormone produced by the pancreas in response to rising blood glucose. Its primary function is to facilitate the movement of glucose from the bloodstream into cells — particularly skeletal muscle cells, fat cells, and liver cells — where it can be used for energy or stored for later use.
When cells respond efficiently to insulin, blood sugar rises after a meal and returns to baseline within approximately two hours. The pancreas produces a moderate amount of insulin. Appetite signals function reliably. Energy is stable between meals.
According to the National Institute of Diabetes and Digestive and Kidney Diseases, insulin resistance describes a state where cells in the muscles, fat, and liver do not respond well to insulin and cannot easily absorb glucose from the blood [5]. When cellular insulin sensitivity declines, the pancreas compensates by producing more insulin to achieve the same glucose clearance. Blood sugar may remain normal — for years — while insulin rises progressively in the background.
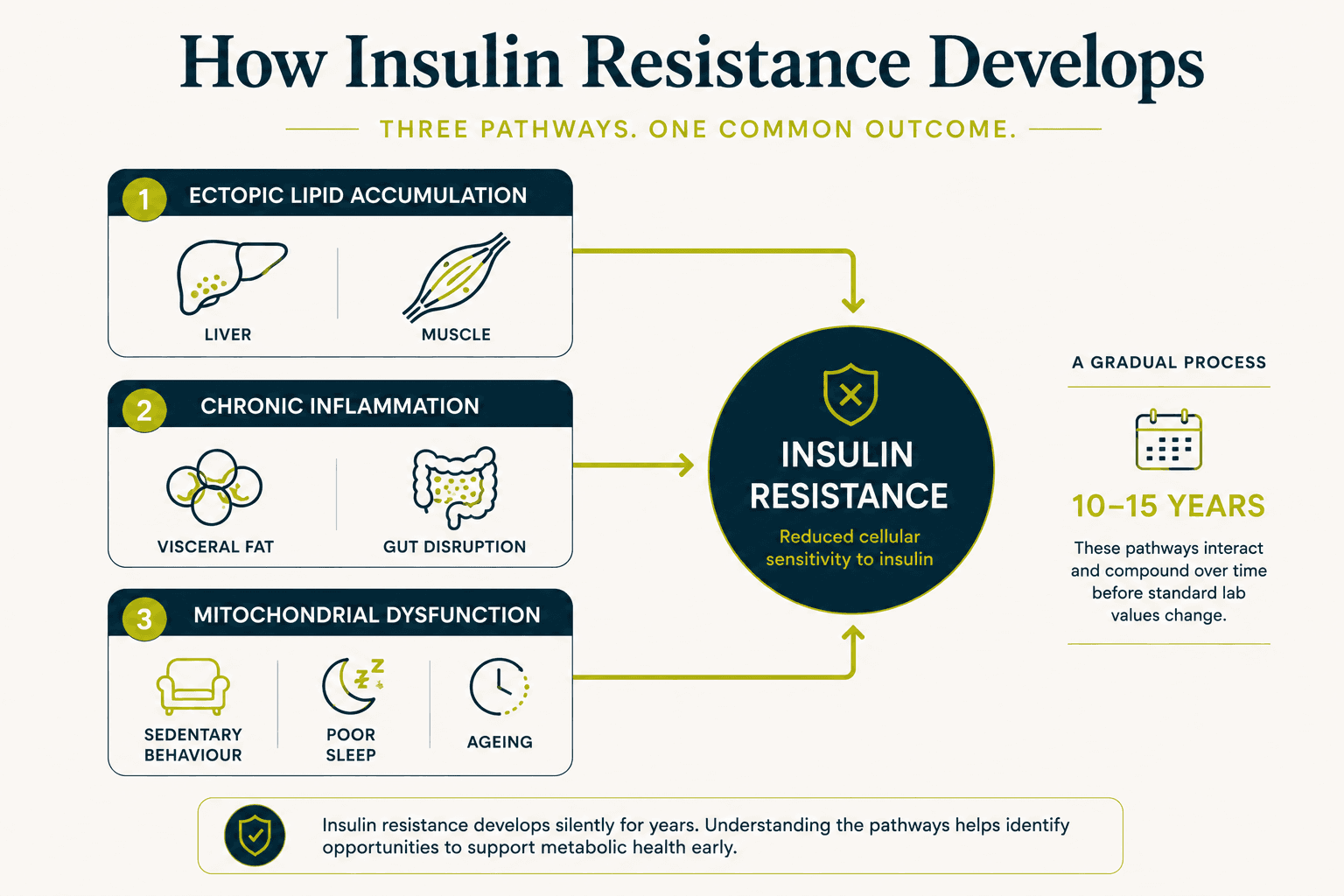
How insulin resistance develops: the 10–15 year mechanism
Insulin resistance does not appear suddenly. It develops through a slow, compounding process that research published in Physiological Reviews(2018) has mapped across three primary pathways (Petersen & Shulman, PMID 30067154) [1]:
Ectopic lipid accumulation
When fat accumulates in the liver (hepatic steatosis) and skeletal muscle, it directly impairs the insulin signalling cascade inside those cells. Ectopic fat — fat stored in organs and muscle rather than in subcutaneous adipose tissue — is metabolically toxic in ways that subcutaneous fat is not. It can accumulate in people with normal BMI.
Chronic low-grade inflammation
Visceral fat — fat stored around the abdominal organs — secretes inflammatory cytokines that interfere with insulin receptor signalling throughout the body. Chronic inflammation driven by visceral fat accumulation, gut microbiome disruption, and ultra-processed food consumption progressively impairs insulin sensitivity over years.
Mitochondrial dysfunction
Mitochondria are the cellular structures responsible for converting glucose and fat into energy. When mitochondrial function declines — driven by sedentary behaviour, poor sleep, chronic stress, and ageing — cells cannot process glucose efficiently and insulin sensitivity deteriorates.
The combination of these three pathways typically takes 10 to 15 years to produce abnormal fasting glucose values. During most of that period, a standard annual physical finds nothing to act on.
The 10-year gap: fasting insulin versus fasting glucose
The most clinically significant fact about insulin resistance is the gap between when it becomes detectable — through fasting insulin — and when it becomes apparent in standard panels through fasting glucose.
A prospective cohort study of 8,143 adults followed over 15 years found that elevated fasting insulin predicted cardiovascular disease onset approximately 10 years earlier than elevated fasting glucose (Salazar et al., Atherosclerosis, 2020 — PMID 24132974) [2]. This is the 10-year gap. Fasting insulin rises. Fasting glucose looks normal. No clinical flag is raised. A decade passes. Then fasting glucose begins to rise — and the conversation about prediabetes begins, a decade after it could have.
Standard panels measure glucose. Insulin is the more sensitive marker. The test exists, is inexpensive, and is almost never ordered.
What causes insulin resistance to develop
The drivers of insulin resistance across the 10–15 year developmental window are consistent across the research literature:
Visceral fat accumulation
The accumulation of fat around the abdominal organs — not total body weight — is the most directly measurable driver of insulin resistance. Waist circumference is a more predictive marker of insulin resistance than BMI. This is why insulin resistance appears across all weight categories: it is a fat location and fat quality problem, not simply a fat quantity problem.
Ultra-processed food consumption
Diets high in refined carbohydrates, industrial seed oils, and ultra-processed foods chronically elevate blood sugar, promote ectopic fat accumulation, and suppress GLP-1 function — accelerating the development of insulin resistance through multiple pathways simultaneously.
Chronic sleep disruption
Sleep deprivation impairs insulin sensitivity acutely — a single poor night of sleep produces measurable next-day insulin resistance. Chronic sleep disruption maintains this effect persistently, becoming one of the most potent accelerants of insulin resistance development over time.
Sedentary behaviour
Skeletal muscle is the primary site of insulin-mediated glucose uptake. When muscle is not regularly challenged through movement, its capacity for glucose uptake declines — directly reducing whole-body insulin sensitivity. Loss of muscle mass with age compounds this effect.
Chronic psychological stress
Cortisol elevates blood sugar independently of diet, promotes ectopic fat accumulation, and impairs insulin signalling at the cellular level. Chronic stress is a direct driver of insulin resistance — not a secondary consideration.
How insulin resistance affects all five signal domains
Insulin resistance is not a single-domain problem. Its effects ripple across all five metabolic signal domains simultaneously.
Energy & Blood Sugar Control
This is the primary domain affected. As insulin resistance progresses, blood sugar takes longer to clear after meals, glucose spikes become more pronounced, and the energy crashes and cravings associated with blood sugar volatility intensify.
Appetite & Hunger Signals
Insulin resistance impairs GLP-1 function and leptin sensitivity — the two primary hormonal mechanisms governing satiety. Food noise, persistent hunger after meals, and amplified cravings are all downstream effects of insulin resistance on appetite signalling.
Digestion & Gut Health
Gut microbiome disruption both contributes to and is worsened by insulin resistance. The gut's capacity to produce GLP-1 declines as microbiome diversity decreases — creating a feedback loop between gut health and insulin sensitivity.
Sleep & Recovery
The relationship is bidirectional: insulin resistance impairs sleep quality, and poor sleep accelerates insulin resistance. This feedback loop is one of the most important — and most often underestimated — drivers of metabolic decline.
Hormones & Stress Response
Insulin resistance elevates cortisol, and cortisol elevates insulin resistance. This is another bidirectional loop: stress impairs insulin sensitivity, and metabolic dysfunction increases the physiological stress burden.
Insulin resistance and metabolic syndrome
Insulin resistance is the common upstream mechanism connecting metabolic dysfunction to metabolic syndrome — and to the most prevalent chronic conditions of modern life.
The American Heart Association defines metabolic syndrome as the presence of three or more of five criteria: abdominal obesity, elevated triglycerides, reduced HDL cholesterol, elevated blood pressure, and elevated fasting glucose. Each of these criteria is a downstream consequence of insulin resistance. The syndrome is the collection of signals that appear after years of progressive insulin resistance — not the cause, but the clinical expression of it (Grundy et al., Circulation, 2005 — PMID 16157765) [3].
Type 2 diabetes represents a further progression: the pancreas, having compensated for declining insulin sensitivity by producing more and more insulin for years, eventually cannot maintain sufficient production. Blood sugar rises permanently above threshold. The diagnosis arrives — often a decade or more after the insulin resistance that caused it was measurable.
How to identify insulin resistance early
The most sensitive early indicators of insulin resistance are:
Fasting insulin
Not routinely included in standard panels. An elevated fasting insulin — even with normal fasting glucose — is the most direct early signal. Clinical interpretation requires a qualified clinician.
Triglyceride-to-HDL ratio
Calculated from standard lipid panel results. A ratio above 2 correlates strongly with elevated fasting insulin and visceral fat accumulation in prospective research.
Waist circumference
The most directly measurable indicator of visceral fat accumulation. Above 102cm in men or 88cm in women indicates elevated risk independent of BMI.
Experiential signals
Afternoon energy crashes, food noise, cravings disproportionate to caloric intake, poor sleep quality, and stress-driven eating are all experiential expressions of insulin resistance across the five signal domains — years before any lab marker crosses a threshold.
The BeyondGLP Metabolic Assessment evaluates all five signal domains — Appetite & Hunger Signals, Energy & Blood Sugar Control, Digestion & Gut Health, Sleep & Recovery, and Hormones & Stress Response — through a structured self-reported profile, producing a personalised MetaScore that identifies which signals may need attention. It does not replace clinical evaluation or laboratory testing.
Check Your Metabolic Profile →
Free · Physician-reviewed · Results in under 5 minutes
Common Questions
Can you have insulin resistance at a normal weight?
Yes. A cross-sectional analysis of 8,721 US adults found that poor metabolic health — including insulin resistance — appeared across all BMI categories, including individuals classified as normal weight (Araújo et al., Metabolic Syndrome and Related Disorders, 2019 — PMID 30484738). Insulin resistance is driven by visceral fat location and quality, not total body weight.
Does insulin resistance always lead to type 2 diabetes?
Not inevitably — insulin resistance can be present for years without progressing to type 2 diabetes. Progression depends on the degree of insulin resistance, the compensatory capacity of the pancreas, and the degree to which the driving factors (visceral fat, sleep disruption, stress, diet quality) are addressed. This is an area where early intervention changes outcomes. Your clinician can advise on your specific risk picture.
Is insulin resistance the same as prediabetes?
They are related but not identical. According to the National Institute of Diabetes and Digestive and Kidney Diseases, prediabetes is a condition where blood sugar levels are higher than normal but not yet high enough to be classified as type 2 diabetes. Insulin resistance is the underlying mechanism that drives prediabetes. Significant insulin resistance can be present years before blood sugar rises enough to qualify as prediabetes.
Can insulin resistance be detected without a blood test?
The experiential signs — afternoon energy crashes, food noise, persistent hunger after meals, changing body composition toward the waist — are reliable pattern signals of insulin resistance in the absence of lab testing. They are not diagnostic, but they are informative. The BeyondGLP Metabolic Assessment is designed to identify these signal patterns systematically.
What is the most useful single addition to a standard blood panel for detecting insulin resistance early?
Fasting insulin is the most sensitive early marker that is almost never routinely included. The triglyceride-to-HDL ratio can be calculated from any standard lipid panel at no additional cost. Waist circumference requires a tape measure. All three together provide a substantially more complete early picture than fasting glucose alone. Clinical interpretation requires a qualified clinician.
Scientific References
- 1.Petersen MC, Shulman GI. Mechanisms of insulin resistance: cellular and molecular pathways. Diabetologia, 2021. PMID 30067154. pubmed.ncbi.nlm.nih.gov/30067154/
- 2.Salazar MR, Carbajal HA, Espeche WG, et al. Fasting insulin as a marker to predict the onset of cardiometabolic diseases: a 15-year prospective study. Atherosclerosis, 2020. PMID 24132974. pubmed.ncbi.nlm.nih.gov/24132974/
- 3.Grundy SM, Cleeman JI, Daniels SR, et al. Diagnosis and management of the metabolic syndrome. Circulation, 2005. PMID 16157765. pubmed.ncbi.nlm.nih.gov/16157765/
- 4.Araújo J, Cai J, Stevens J. Prevalence of optimal metabolic health in American adults: National Health and Nutrition Examination Survey 2009–2016. Metabolic Syndrome and Related Disorders, 2019. PMID 30484738. pubmed.ncbi.nlm.nih.gov/30484738/
- 5.National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), National Institutes of Health. Insulin Resistance and Prediabetes. www.niddk.nih.gov/health-information/diabetes/overview/what-is-diabetes/prediabetes-insulin-resistance
Take the Metabolic Assessment →
See which of your five signal domains may need attention
Educational only. This page is for general education and is not medical advice, diagnosis, or treatment. Always consult a qualified healthcare provider regarding medical decisions. No outcomes are promised — individual results vary. The BeyondGLP Metabolic Assessment is an educational metabolic profile, not a diagnostic device. Reviewed by Dr. Steven Gabriel MD on June 2026.