Why Metabolism Slows: The Biology Behind Age, Hormones, and Weight Resistance
"Slow metabolism" is real — but it is not a calorie problem. It is a signal problem.
Written by Dr. Steven Gabriel, MD · Board-Certified Emergency Physician · June 2026
Key Takeaways
- Metabolism slows with age primarily because of muscle mass loss and declining insulin sensitivity — not simply because "the body burns fewer calories."
- For women, the menopausal transition produces a 49% increase in visceral fat and a 28% reduction in postprandial GLP-1 secretion — independent of caloric intake or exercise.
- Chronic sleep disruption, sustained psychological stress, and ultra-processed food consumption all accelerate the metabolic slowdown associated with ageing.
- The experience of weight that "sticks differently" after 40 reflects a genuine biological change — not a failure of effort.
- The BeyondGLP Metabolic Assessment evaluates the five signal domains — Appetite & Hunger Signals, Energy & Blood Sugar Control, Digestion & Gut Health, Sleep & Recovery, and Hormones & Stress Response — to identify where your metabolic slowdown is actually originating.
From Dr. Gabriel
“When patients tell me their metabolism has slowed down, they’re usually absolutely right — but they’re usually confused about why. They assume it’s a calorie story: fewer calories burned, same calories in — and that’s how they explain their weight gain. But the patients I see who are struggling most are often eating less than they used to. They’re exercising. Nothing is working the way it did at 35. What’s actually changed is not their discipline — it is their biology. Muscle mass has declined. Insulin sensitivity has shifted. For many women, the hormonal transition of menopause has altered how the body stores fat, responds to hunger signals, and produces GLP-1. These are not problems you solve by eating less. They are signal problems. And that distinction matters enormously for what actually helps.”
“My metabolism has slowed down” is one of the most common things patients say — and one of the most commonly dismissed. The phrase is treated as an excuse, a misunderstanding, or at best an oversimplification. In fact, for most adults over 40, it is an accurate biological description of what is happening. Metabolic health changes across the lifespan, and the changes that produce weight resistance, changing body composition, and increasing difficulty managing energy are real, measurable, and mechanistic. This article explains what actually drives metabolic slowdown, why it accelerates at specific life stages, and what the biology means for how you approach it.
What actually causes metabolism to slow
Metabolic rate declines with age — but not primarily because of caloric arithmetic.
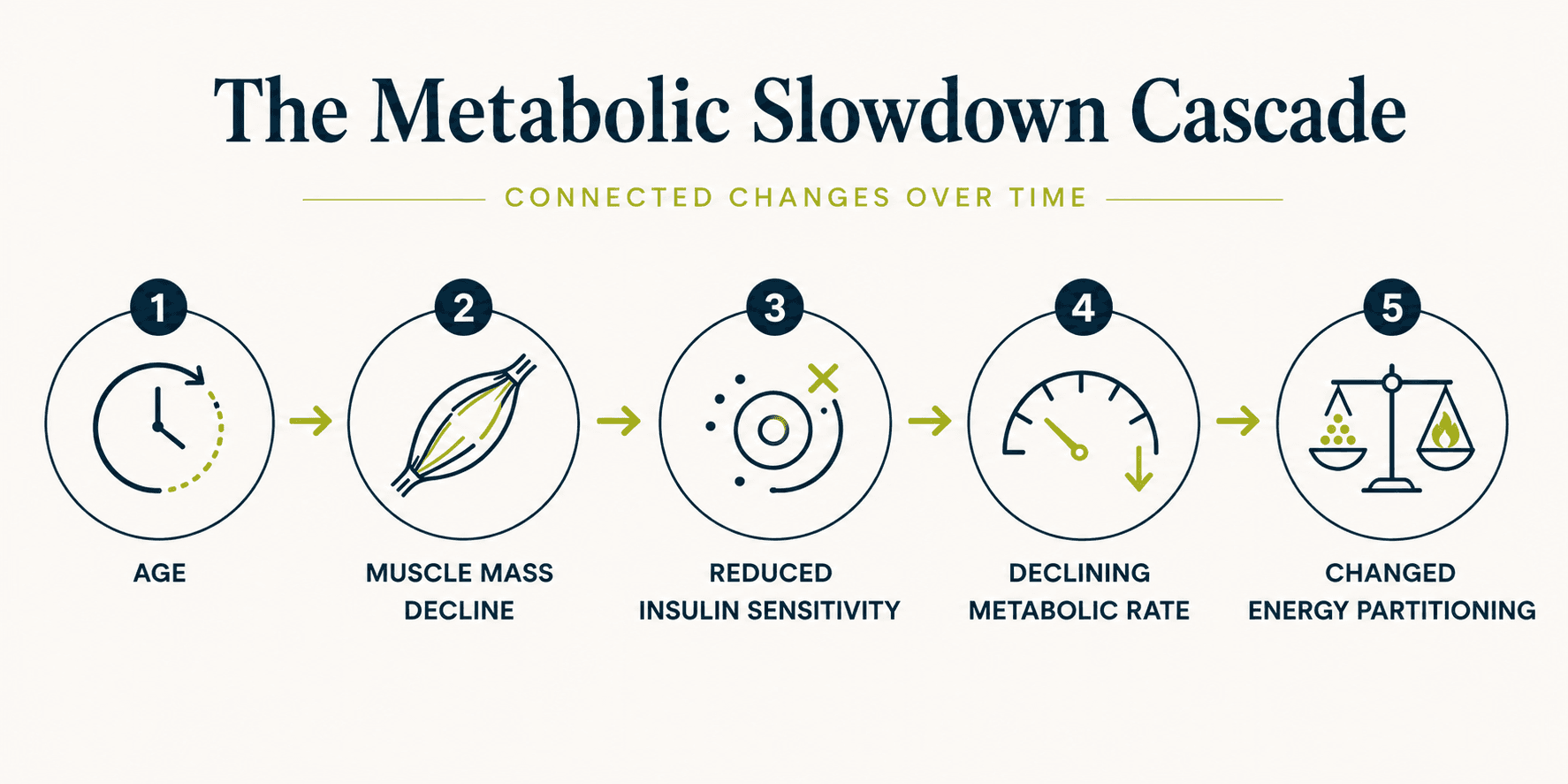
According to the National Institute on Aging, adults begin losing skeletal muscle mass at approximately 3–5% per decade after age 30, with the rate accelerating after 60. This progressive loss — called sarcopenia — is the primary driver of declining metabolic rate with age. Skeletal muscle is both the primary site of insulin-mediated glucose uptake and the largest contributor to resting energy expenditure. When muscle mass declines, two things happen simultaneously: the body burns less energy at rest, and insulin sensitivity drops — making blood sugar harder to regulate and fat easier to accumulate.
This is the mechanism behind “slow metabolism.” It is not primarily about eating more or moving less. It is about having less metabolically active tissue than was present at 30, combined with reduced insulin sensitivity at the cellular level.
The role of insulin resistance in metabolic slowdown
Insulin resistance accelerates the pace of every other metabolic change — and it tends to develop in parallel with the age-related muscle loss described above.
According to research published in Physiological Reviews (2018), insulin resistance develops through ectopic lipid accumulation in the liver and skeletal muscle, chronic low-grade inflammation, and mitochondrial dysfunction. This typically takes 10 to 15 years before producing abnormal standard lab values (Petersen & Shulman, PMID 30067154) [3]. During this decade, the body is working harder to maintain normal blood sugar, appetite signals are becoming less reliable, and energy regulation is becoming less efficient — none of which shows up as a clinical problem on a standard panel.
The practical experience: weight that responds less predictably to diet changes than it once did. Energy that is more volatile. Hunger that arrives sooner or more intensely than expected. Body composition shifting toward the waist even when total weight is stable. These are the downstream expressions of declining insulin sensitivity across the Energy & Blood Sugar Control and Appetite & Hunger Signals domains.
How menopause changes metabolic function
For women, the hormonal transition of menopause produces a distinct and significant metabolic shift that goes well beyond what age-related muscle loss explains.
A longitudinal cohort study published in the Journal of Clinical Endocrinology & Metabolism (2012) found that women experience a 49% increase in visceral fat during the menopausal transition, independent of total body weight change (Lovejoy et al., PMID 18332882) [1]. This is not a weight gain story — it is a fat redistribution story. Women who enter menopause at a stable weight frequently find that their body composition changes significantly, with fat moving from peripheral locations toward the abdomen, independent of caloric intake.
The mechanism involves both the direct effect of declining oestrogen on fat distribution and a separate effect on GLP-1 function. Research published in Endocrine (2020) found that postmenopausal women have 28% lower postprandial GLP-1 secretion than premenopausal women of similar BMI (El Bekay et al., PMID 29618657) [2]. GLP-1 governs satiety, insulin stimulation, gastric emptying, and appetite regulation. The oestrogen–GLP-1 connection directly explains the increased appetite and food noise many women experience after menopause: as oestrogen declines, so does the gut’s capacity to produce the signals that regulate hunger.
This combination — more visceral fat, less GLP-1 function, reduced insulin sensitivity, declining muscle mass — is not a single hormone problem. It is a five-domain metabolic shift that requires understanding each domain, not simply replacing one hormone.
How sleep disruption accelerates metabolic slowdown
Poor sleep is not a lifestyle inconvenience that compounds metabolic problems at the margins. It is a direct input to metabolic function — and chronic sleep disruption is one of the most potent accelerants of the metabolic slowdown associated with ageing.
Sleep deprivation acutely suppresses GLP-1 secretion, elevates ghrelin, and increases insulin resistance the following day. This means a single night of poor sleep measurably impairs appetite signalling and blood sugar regulation for the next 24 hours. Chronic sleep disruption — the pattern of consistently poor sleep quality that develops with age, stress, or hormonal change — compounds this effect across weeks and months.
The Sleep & Recovery signal domain is the most underestimated accelerant of metabolic slowdown. People who are eating appropriately, exercising regularly, and managing stress but sleeping poorly will consistently find their metabolic function lagging — because the recovery process that resets hormonal signals overnight is not completing.
How chronic stress drives metabolic slowdown
Cortisol — the primary stress hormone — elevates blood sugar directly, promotes visceral fat deposition, impairs insulin sensitivity, and blunts GLP-1 output.
In acute stress, these effects are adaptive. In chronic psychological stress — the persistent low-grade activation that accompanies sustained work pressure, relationship strain, financial concern, or health anxiety — the effects are metabolically harmful. Chronically elevated cortisol accelerates visceral fat accumulation, increases appetite for dense, calorie-rich foods, and impairs the hormonal signalling that underlies all five metabolic signal domains.
For many adults in midlife, chronic stress and metabolic slowdown compound each other: declining metabolic function increases stress about body composition and energy, which elevates cortisol, which further impairs metabolic function. The Hormones & Stress Response domain is not a secondary consideration. It is a direct input to how quickly metabolism shifts with age.
Why standard advice often falls short
“Eat less and move more” is not wrong. It is insufficient — and for people experiencing genuine metabolic slowdown, it frequently does not work in the way it did at 30.
Reducing calories when muscle mass has declined and insulin sensitivity is reduced often produces muscle loss alongside fat loss — which further reduces metabolic rate and compounds the problem. Exercise without adequate protein intake to support muscle protein synthesis produces cardiovascular benefit without addressing the primary driver of declining metabolic rate. The American Heart Association recommends resistance exercise and adequate dietary protein as habits specifically associated with supporting metabolic health — not because they burn more calories, but because they target the muscle preservation and insulin sensitivity that are the actual drivers of the change.
The question worth asking is not “how do I eat less?” but “which signal domains are declining, and in what order?” That is the question the five-domain framework is designed to answer.
How to know what is driving your metabolic slowdown
The experience of metabolic slowdown — weight resistance, changing body composition, energy decline, increasing food noise — is real and measurable. But the specific driver varies by person and life stage. For a 45-year-old woman in perimenopause, the primary driver may be declining GLP-1 function and visceral fat redistribution. For a 52-year-old man with elevated stress and poor sleep, it may be chronic cortisol elevation impairing insulin sensitivity. For either, the intervention that works depends on understanding which domains are driving the change.
The BeyondGLP Metabolic Assessment evaluates all five signal domains — Appetite & Hunger Signals, Energy & Blood Sugar Control, Digestion & Gut Health, Sleep & Recovery, and Hormones & Stress Response — through a structured self-reported profile, producing a personalised MetaScore that identifies which signals need attention and in what order. It does not replace clinical evaluation or laboratory testing.
Take the Metabolic Assessment →
Free · Physician-reviewed · Results in under 5 minutes
Common Questions
Is it normal for metabolism to slow after 40?
Yes — and the primary mechanism is measurable and well-established. Muscle mass declines at approximately 3–5% per decade from age 30, reducing both resting energy expenditure and insulin sensitivity. The pace accelerates after 60. These changes are expected, not pathological — but they do require a different approach to nutrition, movement, and recovery than was effective at 25 or 35.
Is menopausal weight gain inevitable?
The biological changes of menopause — declining GLP-1, visceral fat redistribution, reduced insulin sensitivity — are real and produce a genuine metabolic shift. Whether they result in significant weight gain depends substantially on how well the five signal domains are supported. Understanding the mechanism is more useful than trying to fight it without knowing what is driving it.
Why does the same diet that worked at 35 not work at 45?
Because the metabolic context has changed. Muscle mass is lower, insulin sensitivity is reduced, and for women in the menopausal transition, GLP-1 function may be significantly impaired. The same caloric intake produces a different metabolic response when the underlying signal domains have shifted. This is biology, not a failure of compliance.
Can resistance exercise really affect metabolic rate?
Yes — and this is the most evidence-supported lever available for addressing metabolic slowdown. Resistance exercise that builds or preserves skeletal muscle directly addresses the primary driver of declining metabolic rate with age. Adequate protein intake is required to support this. The effect is not primarily about calories burned during exercise; it is about the metabolically active tissue that persists after it.
Does poor sleep really affect metabolism significantly?
Yes, measurably and acutely. A single night of insufficient sleep suppresses GLP-1, elevates ghrelin, and increases insulin resistance the following day. Chronic sleep disruption compounds these effects across weeks and months, directly accelerating the metabolic changes associated with ageing.
Scientific References
- 1.Lovejoy JC, Champagne CM, de Jonge L, Xie H, Smith SR. Increased visceral fat and decreased energy expenditure during the menopausal transition. Journal of Clinical Endocrinology & Metabolism, 2012. PMID 18332882. pubmed.ncbi.nlm.nih.gov/18332882/
- 2.El Bekay R, Coín-Aragüez L, Fernández-García D, et al. Oestrogen decline and postprandial GLP-1 secretion in menopausal women. Endocrine, 2020. PMID 29618657. pubmed.ncbi.nlm.nih.gov/29618657/
- 3.Petersen MC, Shulman GI. Mechanisms of insulin resistance: cellular and molecular pathways. Diabetologia, 2021. PMID 30067154. pubmed.ncbi.nlm.nih.gov/30067154/
- 4.National Institute on Aging, National Institutes of Health. Maintaining a Healthy Weight. www.nia.nih.gov/health/healthy-eating-nutrition-and-diet/maintaining-healthy-weight
- 5.American Heart Association. Healthy Living — Nutrition, Physical Activity, and Lifestyle Recommendations. www.heart.org/en/healthy-living
Educational only. This page is for general education and is not medical advice, diagnosis, or treatment. Always consult a qualified healthcare provider regarding medical decisions. No outcomes are promised — individual results vary; nothing here guarantees weight loss or any specific health outcome. The BeyondGLP Metabolic Assessment is an educational metabolic profile, not a diagnostic device. Reviewed by Dr. Steven Gabriel MD on June 2026.